CE / CME
Physician Assistants/Physician Associates: 1.50 AAPA Category 1 CME credits
Pharmacists: 1.50 contact hours (0.15 CEUs)
Nurse Practitioners/Nurses: 1.50 Nursing contact hours
Physicians: maximum of 1.50 AMA PRA Category 1 Credits™
Released: April 09, 2025
Expiration: October 08, 2025
BREAKWATER: First-line Encorafenib + Cetuximab + Chemotherapy vs SoC for BRAF V600E–Mutant mCRC
Christopher Lieu, MD, FASCO:
BREAKWATER was a phase III study of first-line EC with or without mFOLFOX6 chemotherapy vs physician’s choice SoC chemotherapy for BRAF V600E–mutated mCRC.1 EC was approved by the FDA in 2020 for adults with refractory mCRC with a BRAF V600E mutation,2,3 and this treatment combination has been in practice for several years now. Primary endpoints were ORR by blinded independent central review (BICR) and PFS, and secondary endpoints were overall survival (OS) and safety.
BREAKWATER: Baseline Characteristics
Christopher Lieu, MD, FASCO:
Baseline characteristics, including age, sex, Eastern Cooperative Oncology Group (ECOG) performance status (PS), and number of organs involved, were very similar between the experimental arm and SoC arm.1
BREAKWATER: Response by BICR
Christopher Lieu, MD, FASCO:
In patients receiving EC plus mFOLFOX6, the ORR was 60.9% vs 40.0% in patients receiving SoC, a statistically significant and clinically meaningful improvement, with a P value of .0008. There was considerable stable disease in both arms, but more partial responses in the EC plus mFOLFOX6 arm vs the SoC arm (58.2% vs 38.2%, respectively).1
BREAKWATER: ORR by Subgroup
Christopher Lieu, MD, FASCO:
The ORR benefit of EC plus mFOLFOX6 was consistent across all subgroups, regardless of tumor side (left-sided tumor or right-sided tumor), number of organs involved, ECOG PS at baseline, and the presence of liver metastases.1
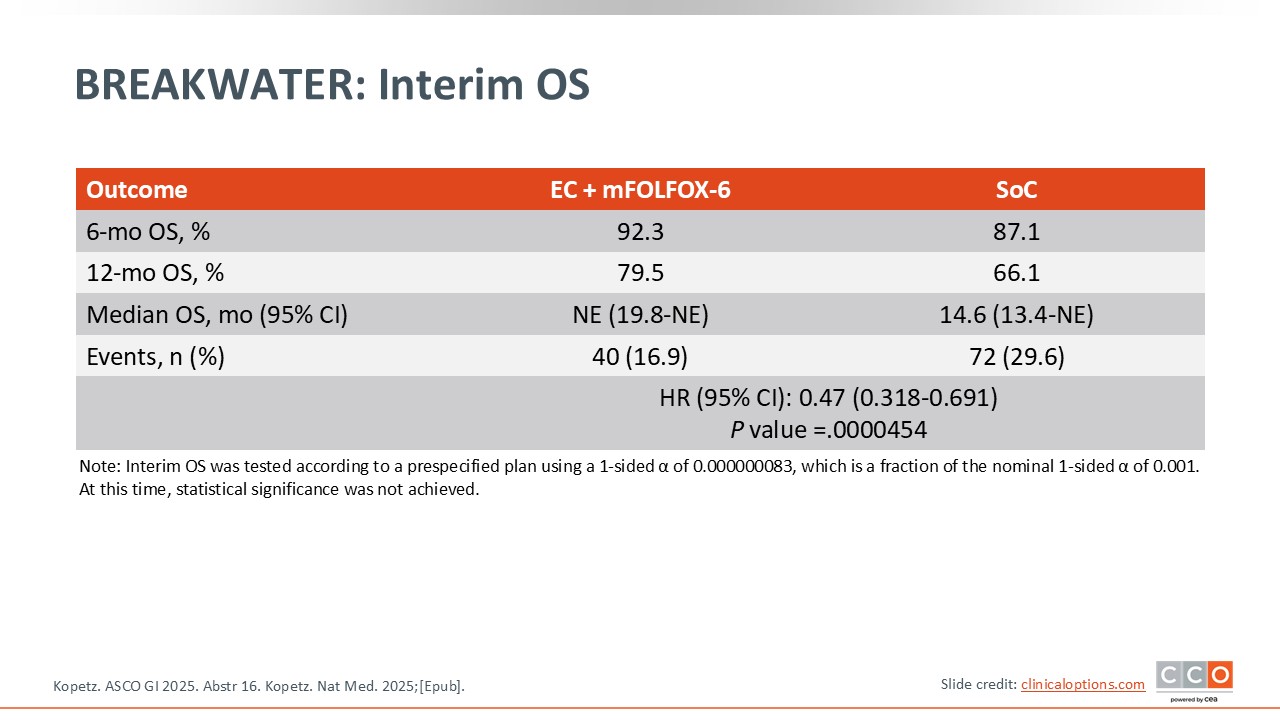
BREAKWATER: Interim OS
Christopher Lieu, MD, FASCO:
OS data were immature. Although there was no statistically significant difference in OS between arms, the 12-month OS rate was 79.5% in the treatment arm vs 66.1% in the SoC arm. Again, this was not a statistically significant difference, but you can start to see a separation of the curves already in short-term follow-up.1
BREAKWATER: Safety and Dose Modifications
Christopher Lieu, MD, FASCO:
This table summarizes safety events. The percentages of treatment-emergent adverse events (TEAEs) were very similar between the 2 arms (99.6% in the EC plus mFOLFOX6 arm vs 97.8% in the SoC arm), as were the rates of TRAEs. Both regimens were fairly well tolerated, with no new safety signals observed with the addition of EC.1
BREAKWATER: Most Frequent All-Causality TEAEs
Christopher Lieu, MD, FASCO:
In the EC plus mFOLFOX6 vs SoC arm, the most frequent TEAEs were nausea (51.1% vs 48.2%, respectively), anemia (36.4% vs 22.8%), diarrhea (34.2% vs 46.9%), decreased appetite (33.3% vs 25.0%), and vomiting (33.8% vs 21.1%). With the addition of EC, there was a higher rate of rash, but this is a known on-target effect of EC.1
BREAKWATER: Conclusions
Christopher Lieu, MD, FASCO:
This is a practice-changing study and the FDA approved EC plus mFOLFOX6 chemotherapy for patients with untreated BRAF V600E–mutated mCRC based on these data.2,3 The ORR will further improve, as should OS based on early results. This study shows that adding EC to mFOLFOX6 early has a clinically meaningful impact for patients.
Arvind Dasari, MD, MS:
I completely agree. This study is indeed practice-changing, and all patients with BRAF V600E–mutated mCRC should be receiving first-line EC plus chemotherapy.
Rachna Shroff, MD, MS, FASCO:
I think it will be important now to start thinking about subsequent therapies for these patients and whether there are additional opportunities to better understand resistance and appropriate treatment approaches. This will be an important area for future research.
I think it is wonderful that this regimen is something that can be really offered to newly diagnosed patients with BRAF V600E–mutant mCRC.
Christopher Lieu, MD, FASCO:
I could not agree more. It speaks to the extreme importance of getting biomarker data back quickly and making clinically meaningful decisions based on those data. It is also important to understand that this therapy is strictly for BRAF V600E–mutated mCRC and not other types of BRAF mutations.1
Let’s return to an earlier question.
CAO/ARO/AIO-12 and OPRA: Pooled Analysis of Watch and Wait vs Total Mesorectal Excision in Patients With Rectal Cancer Who Respond to Total Neoadjuvant Therapy
Christopher Lieu, MD, FASCO:
Treatment for rectal cancer has greatly evolved over the past few years, and many patients are now receiving total neoadjuvant therapy that includes chemoradiation followed by chemotherapy, followed by either nonoperative management or surgery if there is residual disease. One major question is whether survival is affected if patients do not proceed with mandatory surgery following the completion of chemoradiation and chemotherapy.
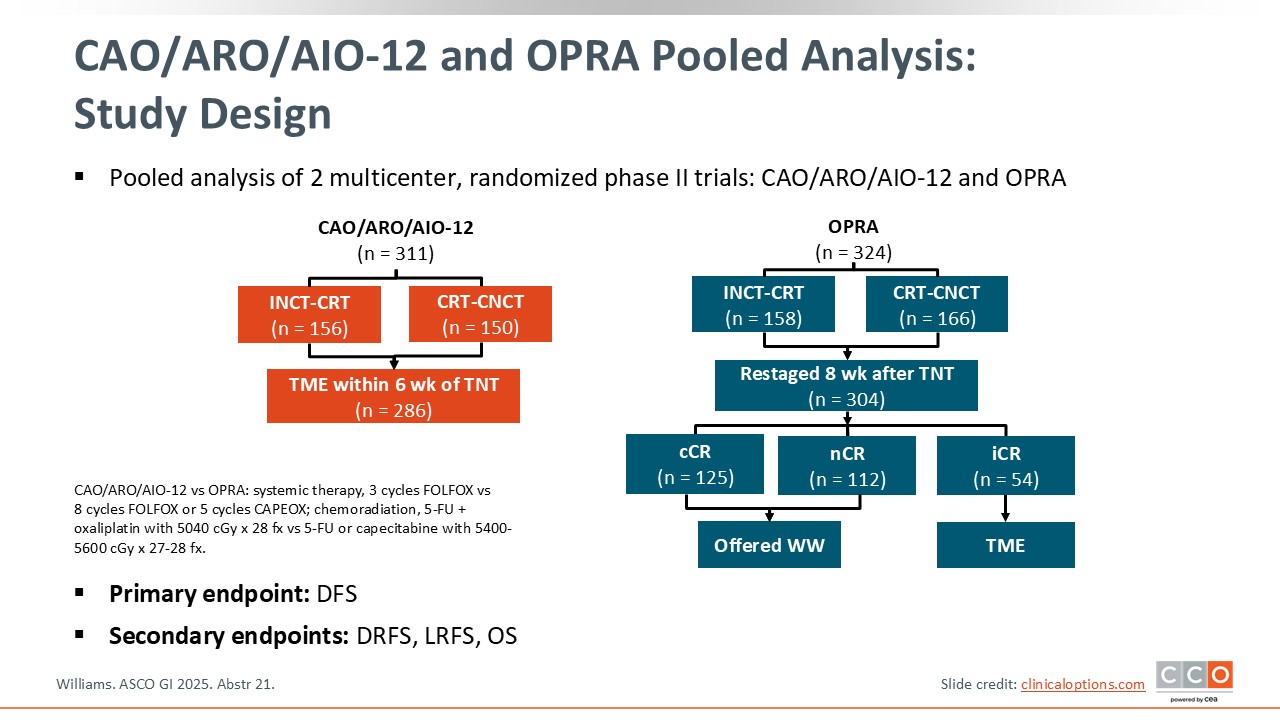
Emerging data indicate that watch and wait is an effective strategy and does not negatively affect survival, and this study really adds to that. This was a pooled analysis of the randomized phase II CAO/ARO/AIO-12 and OPRA trials. This was essentially an analysis of watch and wait vs total mesorectal excision in patients with stage II/III rectal cancer who responded to total neoadjuvant therapy.4
The OPRA study looked at organ preservation rates after total neoadjuvant therapy, and the CAO/ARO/AIO-12 study also used total neoadjuvant therapy, but here, surgery was mandated. The pooled analysis aimed to determine whether surgery improves survival. The primary endpoint was disease-free survival (DFS), and the secondary endpoints were distant recurrence-free survival, local recurrence-free survival, and OS.
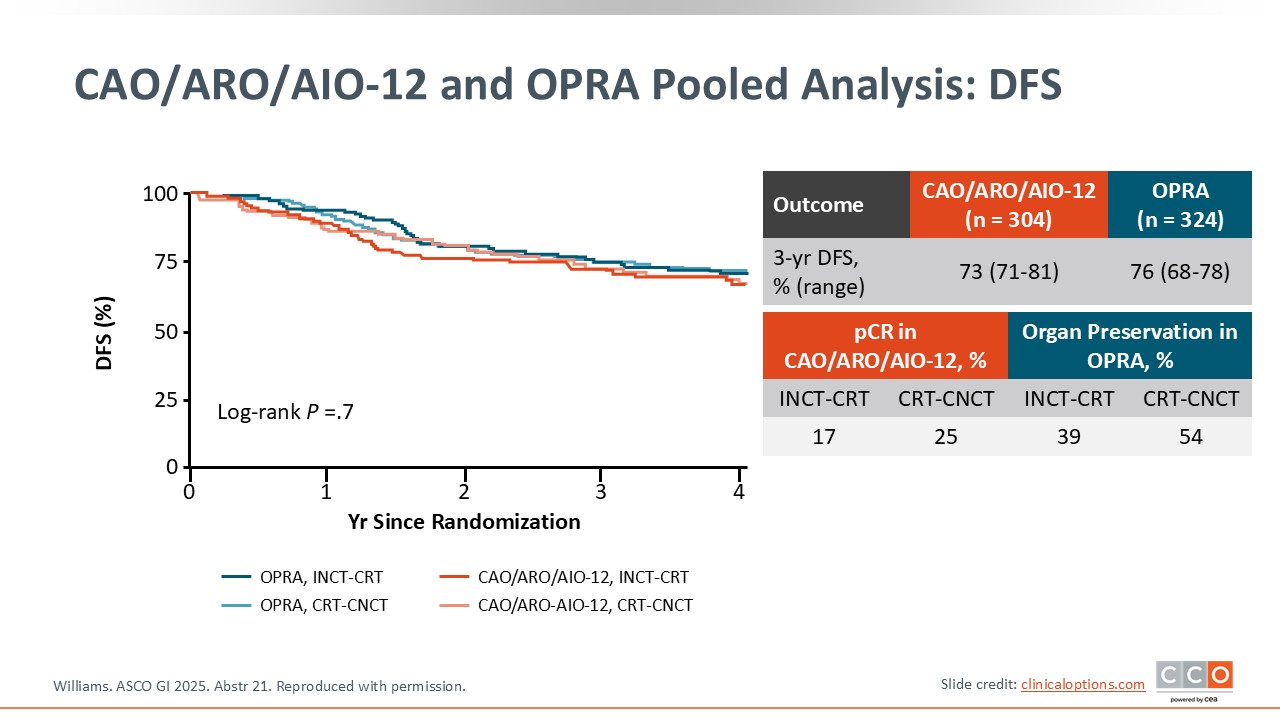
CAO/ARO/AIO-12 and OPRA Pooled Analysis: DFS
Christopher Lieu, MD, FASCO:
Shown here is the Kaplan-Meier DFS curve. The 3-year DFS rate was extremely similar between the 2 studies: 73% in the group treated with surgery and 76% in the group treated with a watch-and-wait approach.4
CAO/ARO/AIO-12 and OPRA Pooled Analysis: Additional Survival
Christopher Lieu, MD, FASCO:
Here are some additional survival data at 3 years. The OS rate was 92% in the surgery group and 94% in the watch-and-wait group. The distant recurrence-free survival and local recurrence-free survival rates were also similar (82% and 95%, respectively), with no statistically significant differences between groups.4
CAO/ARO/AIO-12 and OPRA Pooled Analysis: Conclusions
Christopher Lieu, MD, FASCO:
This study adds to the emerging data from the International Watch & Wait Database, showing that in the select group of patients who have a near complete response (nCR) or a complete response (CR) to total neoadjuvant therapy, a watch-and-wait strategy is 1) viable, 2) does not seem to affect survival in a meaningful way, and 3) allows patients to avoid surgery, which has significant advantages.
There are some limitations regarding this type of analysis. This is an analysis across 2 different trials with different treatment regimens, including different chemotherapy and radiation regimens. In the CAO/ARO/AIO-12 study, only 3 cycles of FOLFOX were given,5 whereas in OPRA, 8 cycles of FOLFOX or 5 cycles of capecitabine and oxaliplatin were given.6 It can be difficult to do these cross-trial comparisons, particularly when there may be differences between patient populations and in treatment. However, I think these data indicate similar outcomes between surgery and watch and wait in this specific group of patients.
Arvind Dasari, MD, MS:
I completely agree, and I think it would be very challenging to perform a randomized study of watch and wait vs surgery, given the strong preference that patients and their families have for watch and wait if they achieve a CR or an nCR. Thinking about the bigger picture, it is amazing to see how rectal cancer management is rapidly evolving from trimodal therapy (ie, chemotherapy, radiation, and surgery) to tailoring modalities based on biomarker status, for instance, in patients with MSI-H rectal cancer who may prefer the watch-and-wait approach.
Rachna Shroff, MD, MS, FASCO:
I also agree. The improvements in morbidity associated with these emerging treatments is wonderful to see. I think this analysis further enhances the shift in treatment approach and ultimately helps with clinical decision-making and the ways in which healthcare professionals may approach patients with rectal cancer.4
CheckMate 8HW: Interim Analysis of Phase III Trial of Nivolumab + Ipilimumab vs Nivolumab for MSI-H or dMMR mCRC
Arvind Dasari, MD, MS:
The next study is the international, randomized phase III CheckMate 8HW study of patients with metastatic or advanced CRC with an MSI-H or dMMR status. Patients were randomized to one of 3 arms: nivolumab with or without ipilimumab followed by nivolumab maintenance therapy vs investigator's choice chemotherapy.
The coprimary endpoints were: 1) PFS with nivolumab plus ipilimumab vs nivolumab across multiple lines of therapy, assessed via BICR, which was the focus of this presentation, and 2) PFS of nivolumab plus ipilimumab vs chemotherapy in the frontline setting, which was presented previously and showed the superiority of first-line nivolumab plus ipilimumab over chemotherapy (NCT04008030).7
CheckMate 8HW: Baseline Characteristics
Arvind Dasari, MD, MS:
Overall, the patient characteristics were well balanced between the treatment arms. Approximately 700 patients in total were evaluated. Of note, the majority of patients had not received any previous treatment.7
CheckMate 8HW: PFS (Primary Endpoint)
Arvind Dasari, MD, MS:
Here are the Kaplan-Meier survival curves in patients with centrally confirmed MSI-H/dMMR status. The study showed a statistically significant improvement in median PFS in the nivolumab plus ipilimumab arm vs nivolumab alone arm (not reached vs 39 months, respectively) (HR: 0.62; P = .0003). This survival benefit was consistent in all randomized patients as well, with median PFS durations of 54 vs 18 months for the nivolumab plus ipilimumab vs nivolumab alone arms.7
CheckMate 8HW: PFS by Subgroup
Arvind Dasari, MD, MS:
This PFS benefit was consistent across all subgroups, regardless of the presence of liver metastases, mutation status, and history of Lynch syndrome.7
CheckMate 8HW: ORR, BOR, DoR, and HRQoL
Arvind Dasari, MD, MS:
The response rates, assessed via BICR, also improved with the combination of nivolumab plus ipilimumab vs nivolumab alone. The ORR increased significantly, from approximately 58% to 71% (P = .001).
The mean change in health-related quality of life from baseline improved in both arms, but the nivolumab plus ipilimumab arm reached the prespecified threshold for a meaningful change at Week 21.7
CheckMate 8HW: Safety
Arvind Dasari, MD, MS:
This table shows both TRAEs and immune-mediated adverse events as well as events leading to discontinuation or death in both treatment arms.
There were no new safety signals. The combination was associated with numerically higher rates of TRAEs leading to discontinuation and grade 3/4 TRAEs.
Overall, nivolumab plus ipilimumab appears to be well tolerated, with a slight increase in toxicities compared to nivolumab alone, which is to be expected.7
CheckMate 8HW: Conclusions
Arvind Dasari, MD, MS:
Based on these data, I think nivolumab plus ipilimumab should be considered the new SoC for patients who are MSI-H in the frontline setting over pembrolizumab alone, which is the current SoC.
Rachna Shroff, MD, MS, FASCO:
This was an important follow-up in terms of really understanding the difference between nivolumab alone vs nivolumab plus an anti–CTLA-4 agent. It is not surprising that the combination was beneficial, and it should be the new SoC. What is also reassuring and an added strength of this study is that nivolumab and ipilimumab improved health-related quality of life.
Christopher Lieu, MD, FASCO:
I could not agree more. This is practice changing in the sense that many people were using single-agent immune checkpoint inhibitor therapy for MSI-H patients with mCRC, but patients want long, durable responses. These 3-year PFS rates are significantly higher in the combination arm, and I think many patients are willing to trade off a slightly higher chance of toxicity for a durable response.7
Let’s now return to a question from earlier.
Botensilimab ± Balstilimab for Refractory Microsatellite-Stable Metastatic Colorectal Cancer Without Liver Metastases
Arvind Dasari, MD, MS:
This international, open-label, randomized phase II study evaluated immunotherapy in patients with microsatellite-stable (MSS) mCRC without liver metastases. There were 5 arms, including the SoC arm (TAS-102, a combination of trifluridine and tipiracil, or regorafenib) and 4 experimental arms: 2 with botensilimab (an anti–CTLA-4 antibody) alone at different doses and 2 with botensilimab plus balstilimab (an anti–PD-1 antibody). In total, 234 patients who had received prior chemotherapy but no immunotherapy were randomized to one of these 5 arms.
The primary endpoint was ORR by the investigators. Key secondary endpoints include duration of response, PFS, OS, pharmacokinetics, and safety.8
Botensilimab ± Balstilimab for Refractory MSS mCRC: Baseline Characteristics
Arvind Dasari, MD, MS:
Among the 234 patients enrolled, the baseline characteristics were fairly well balanced across the different arms.8
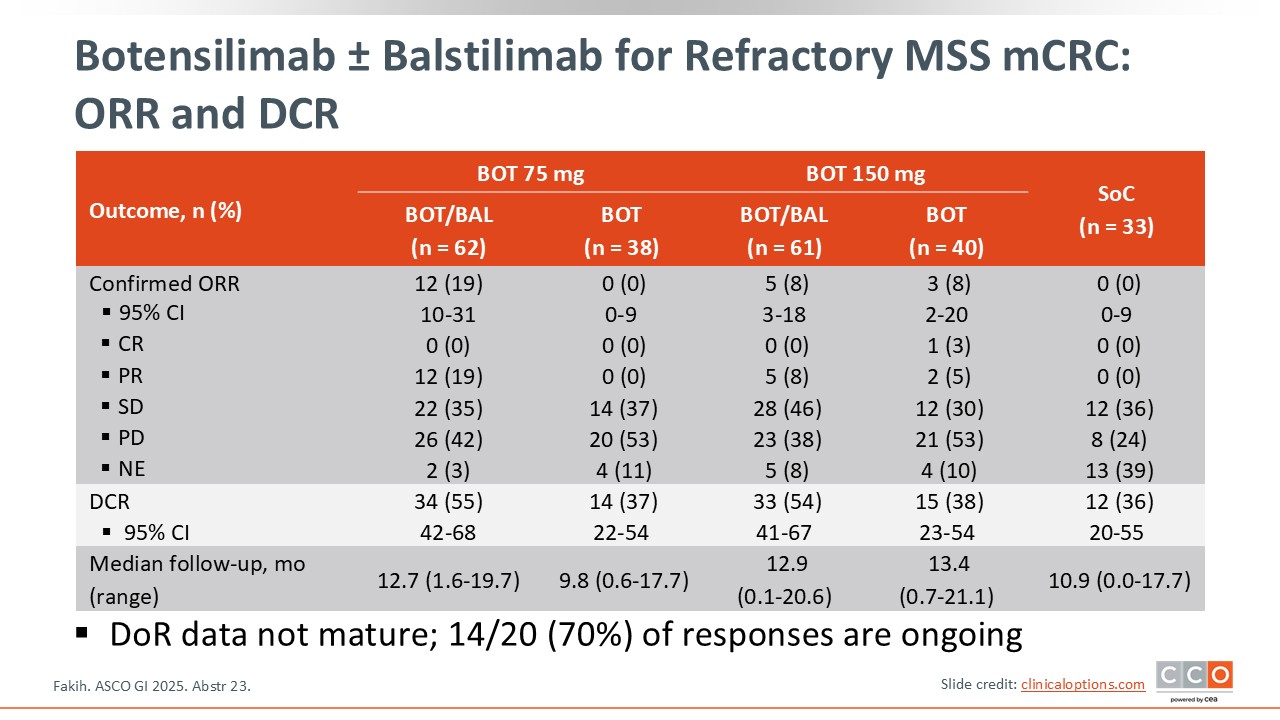
Botensilimab ± Balstilimab for Refractory MSS mCRC: ORR and DCR
Arvind Dasari, MD, MS:
As I mentioned, the primary endpoint was ORR. As to be expected, there were no responses in the SoC arm with either TAS-102 or regorafenib. With botensilimab alone, the responses were fairly minimal in both arms.
What was intriguing was the activity noted with the addition of balstilimab. Surprisingly, there was a numerically higher response rate with the combination at the lower dose of botensilimab. There were no CRs with the combination, but the ORR was 19% in the 75-mg arm vs 8% in the 150-mg arm. The disease control rate (DCR) was also better with the combination regardless of the dose of botensilimab.8
Botensilimab ± Balstilimab for Refractory MSS mCRC: Safety
Arvind Dasari, MD, MS:
Not surprisingly, toxicity was higher with the combination, especially with botensilimab 150 mg. One of the main concerns with this combination, as it was being developed, was the risk of colitis and colitis-related diarrhea. Although there was some guidance around managing this diarrhea and being proactive, a significant proportion of patients did develop toxicities, including diarrhea and colitis, with approximately 27% of the patients in the botensilimab 150 mg combination arm developing grade ≥3 colitis and approximately 18% in the botensilimab 75 mg combination arm.
Regarding any immune-mediated adverse events, approximately 80% of patients in the 150 mg combination arm and approximately 60% in the 75 mg combination arm developed toxicity.8
Botensilimab ± Balstilimab for Refractory MSS mCRC: Conclusions
Arvind Dasari, MD, MS:
Overall, this trial confirmed the activity observed in the phase I trial.9 The results here are not quite as compelling as those seen in that trial, but they do show activity of this regimen in patients with MSS disease. This trial also confirms that this activity seems to be limited to patients without liver metastases, although the reason is unclear, and suggests that a lower dose of botensilimab should be considered.
Overall, these data are intriguing and compelling but not practice changing. These results need to be confirmed with a further phase III trial before this regimen can be considered practice changing.
Christopher Lieu, MD, FASCO:
This is an interesting study because we are starting to see responses in patients with MSS mCRC, which is a significant paradigm change. And it is interesting that the responses were seen in patients without liver metastases, building on the body of evidence suggesting that immunotherapy seems to work better in this subgroup of patients. The response rate is certainly promising. Data on PFS and OS in this cohort will be anxiously awaited. It will also be interesting to see what subsequent studies show regarding maintaining this response rate.
Rachna Shroff, MD, MS, FASCO:
I agree. duration of response was not reported here, but it will be important. I agree that the incidence of grade 3/4 adverse events, specifically colitis, cannot be downplayed. When this moves to a larger phase III study, it will be important to track and understand the trade-off between response, survival, duration, and toxicity.8
STARTER-NET: Everolimus ± Lanreotide for Unresectable or Recurrent GEP-NET
Arvind Dasari, MD, MS:
STARTER-NET was a multicenter, open-label, randomized phase III study of everolimus with or without lanreotide for unresectable or recurrent gastroenteropancreatic neuroendocrine tumors (GEP-NETs). This study enrolled patients with grade 1/2 GEP-NETs that were nonfunctional and advanced with a Ki-67 index of 5% to 20% or those with a Ki-67 index of <5% with diffuse liver metastases with no prior therapy. In total, 178 patients were enrolled.
Patients were randomized to everolimus 10 mg/day plus lanreotide 120 mg/month subcutaneously or everolimus 10 mg/day alone (control arm). The primary endpoint was PFS, and secondary endpoints included ORR, OR, safety, and DCR.10
STARTER-NET: Baseline Characteristics
Arvind Dasari, MD, MS:
Overall, the baseline characteristics were well balanced between the 2 arms. Of note, the pancreas was the primary organ affected in more than two thirds of patients, and approximately 75% of patients had a Ki-67 index ≥5%.10
STARTER-NET: PFS (Primary Endpoint)
Arvind Dasari, MD, MS:
The planned interim analysis was conducted in 145 patients. The median PFS significantly improved from approximately 11.5 months to almost 30.0 months with the combination of everolimus plus lanreotide, with an HR of 0.38 and a P value of .00017. An updated analysis from November 2024, with 23 more patients, confirmed these findings.10
STARTER-NET: PFS by Subgroup
Arvind Dasari, MD, MS:
As shown here, the improvement in median PFS appeared to be consistent across all the subgroups evaluated.10
STARTER-NET: Additional Efficacy Measures
Arvind Dasari, MD, MS:
Of note, the ORR improved significantly, from approximately 8% to 23%, with the addition of lanreotide (P = .011). The DCR was 92% for the combination arm and 85% for the everolimus alone arm. As to be expected for a study in indolent tumors such as NETs, the OS data were not yet mature, with reported 1-year rates of 97.0% and 96.2% in the single-agent and combination arms, respectively.10
STARTER-NET: Safety
Arvind Dasari, MD, MS:
Regarding toxicities, as to be expected, the combination arm had a higher rate of grade ≥3 nonhematologic toxicities, being noted in approximately one third of patients in the combination arm vs approximately 15% in the everolimus alone arm. The most common toxicities occurring in either group were fatigue, diarrhea, oral mucositis, and hyperglycemia (especially with the combination because both can cause hyperglycemia.10
STARTER-NET: Conclusions
Arvind Dasari, MD, MS:
These intriguing data show that the combination of lanreotide plus everolimus appears to be superior to everolimus alone, with an improvement in PFS. However, there were a few drawbacks to this study. First, everolimus, which was used in the control arm, is not something typically used in the frontline setting. Nearly every patient with a NET tends to be started on a somatostatin analog like lanreotide or octreotide, which may have been a better comparator.
Second, in indolent tumors like NETs, the combination may not necessarily provide much benefit because the components could be given sequentially. The increased toxicity with only a slight increase in response rate is also important to note. I would not say the treatment regimen described in this study is practice changing.
Rachna Shroff, MD, MS, FASCO:
It is very important to recognize the impact of tumor type. The indolent nature of this disease, where more is not necessarily better, is important to keep in mind. It will also be important to determine whether the combination of 2 drugs is better than 1 and whether 2 agents act synergistically, not just for NETs but for all tumor types.
Christopher Lieu, MD, FASCO:
I agree that the results are intriguing in the sense that the response rate is fairly impressive considering treatment of an indolent disease. In patients with significant symptoms because of tumor burden, this may be an option.10
Arvind Dasari, MD, MS:
Research into treatment for NETs was prominent at the 2025 ASCO GI meeting. Other interesting studies in NETs included the following:
On March 26, 2025, the FDA approved cabozantinib for adult and pediatric patients 12 years of age or older with previously treated, unresectable, locally advanced or metastatic, well-differentiated pNET and well-differentiated epNET.12 This approval was based on findings from the CABINET trial, which found that in 203 patients with previously treated epNETs, cabozantinib was associated with a median PFS of 8.4 months vs 3.9 months with placebo (HR: 0.38; P <.001); in 95 patients with previously treated pNETs, the median PFS with cabozantinib was 13.8 months vs 4.4 months with placebo (HR: 0.23; P <.001).13
Let’s now return to a question from earlier.
ACCELERATE: Adjuvant Chemotherapy ± Chemoradiation in Gallbladder Cancer
Rachna Shroff, MD, MS, FASCO:
The ACCELERATE study was a multicenter, randomized phase III trial conducted in India that looked only at patients with at least pT2 or node-positive gallbladder cancer who had undergone radical cholecystectomy. Patients were randomized to one of 2 arms. Patients in the investigational arm received physician’s choice of platinum-based chemotherapy: gemcitabine and oxaliplatin or gemcitabine and cisplatin for 3 cycles, followed by a typical course of chemoradiation with capecitabine. Patients in the control arm received 6 cycles of gemcitabine and platinum-based chemotherapy. The primary endpoint was recurrence-free survival (RFS), a typical primary endpoint for adjuvant studies on biliary cancer. It is important to note that initially, the planned number of enrolled patients was closer to 200, but the study had to close early because of low accrual. In total, 94 patients were randomized.14
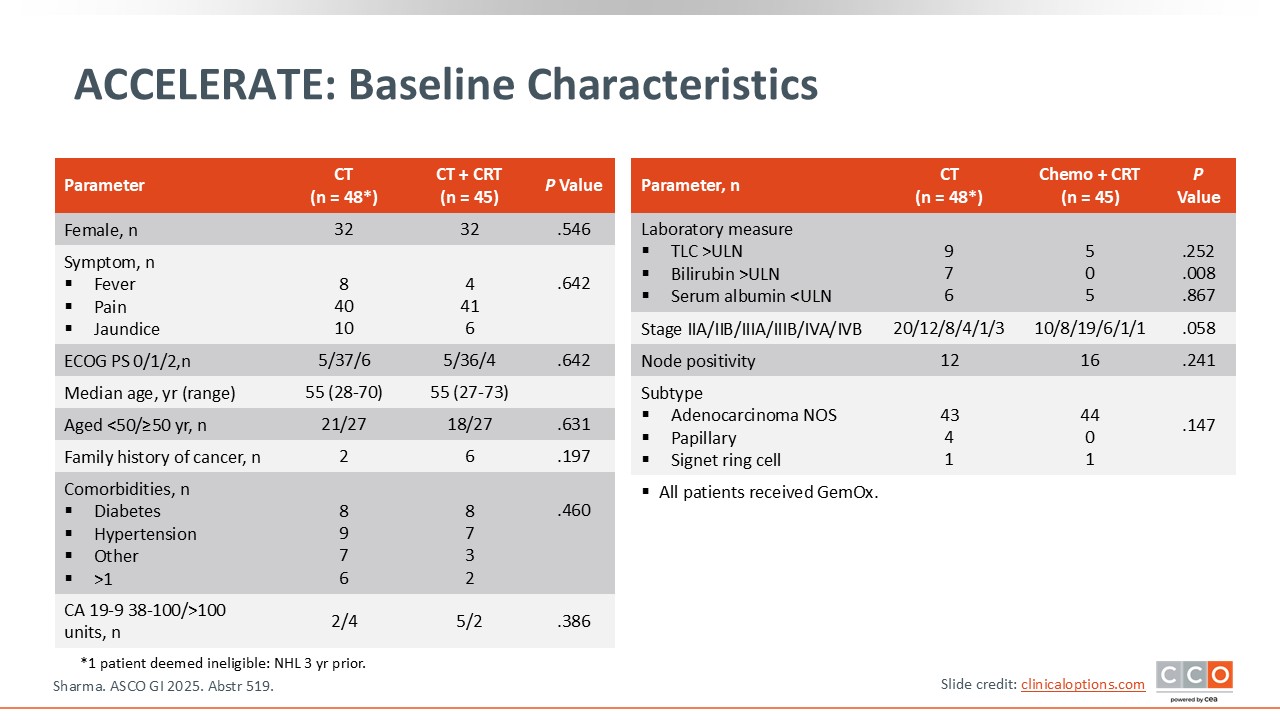
ACCELERATE: Baseline Characteristics
Rachna Shroff, MD, MS, FASCO:
As shown here, the baseline characteristics were relatively well balanced between the 2 arms. Patients had primarily stage IIA, IIB, and IIIA disease. There were no significant differences between arms regarding comorbidities or CA 19-9 levels being >100 units or <100 units.14
ACCELERATE: RFS (Primary Endpoint)
Rachna Shroff, MD, MS, FASCO:
The primary endpoint, RFS, shown here as a Kaplan-Meier curve, did not significantly improve with the addition of chemoradiation (HR: 1.59; P = .156). The median RFS for the chemotherapy arm was 51.96 months vs 43.99 months for the chemotherapy with radiation arm. Sixteen patients in the chemotherapy arm progressed, and 22 in the chemotherapy followed by chemoradiation arm progressed.14
ACCELERATE: RFS by Subgroup
Rachna Shroff, MD, MS, FASCO:
The multivariate analysis demonstrated that node positivity, advanced stage, and high CA 19-9 levels, in addition to ECOG PS, number of chemotherapy cycles, and serum albumin, affected RFS.14
ACCELERATE: OS by Subgroup
Rachna Shroff, MD, MS, FASCO:
When looking at OS, there was no significant improvement with the addition of chemoradiation. Again, survival seemed to be driven by the typical prognostic factors often thought about in gallbladder cancer as well as across biliary tract malignancies, such as node positivity, advanced stage, and high CA 19-9 levels.14
ACCELERATE: Safety
Rachna Shroff, MD, MS, FASCO:
In general, patients who receive gemcitabine and platinum-based chemotherapy followed by gemcitabine and radiation tend to have more toxicities, not only all grades but also grades 3/4. Nothing here was surprising or seemed out of the ordinary. Typical hematologic toxicities, including neutropenia and thrombocytopenia, were notable in both arms. The incidences of diarrhea as well as peripheral neuropathy (all grades) were higher in the chemotherapy alone arm.14
ACCELERATE: Conclusions
Rachna Shroff, MD, MS, FASCO:
The investigators concluded that the addition of chemoradiation to chemotherapy did not improve RFS vs chemotherapy alone. As noted, only 94 patients were enrolled. However, I believe this study adds value. It is important to recognize the differences between gallbladder cancer and intrahepatic and extrahepatic cholangiocarcinomas. The BILCAP study, which set the benchmark for the adjuvant approach in biliary tract cancers, included all 3 different types of biliary cancers, and per the intention-to-treat analysis, RFS did not improve significantly.15
This study was unable to accrue as many patients as planned, which speaks to the fact that it may be difficult to perform adjuvant studies in patients with a biliary anatomical subtype. Of note, patients with node-positive disease are a high-risk patient population at high risk for recurrence. It can be difficult to tease out what additional benefit, if any, radiation could offer.
In addition, gemcitabine and platinum-based chemotherapy is not yet the SoC for adjuvant therapy. The ACTICCA-1 study is currently comparing chemotherapy with gemcitabine and cisplatin to capecitabine and observation (NCT02170090).
Christopher Lieu, MD, FASCO:
I completely agree. It has been interesting in this space where less appears to be more in terms of capecitabine still being the SoC. And many studies have tried to escalate chemotherapy and chemoradiation, but none has shown improved survival. I think the take-home message from this study, along with many others, is that capecitabine should be used as adjuvant therapy. The addition of anything to this regimen is exploratory at this time.
Arvind Dasari, MD, MS:
For these patients, the quality of surgery remains of paramount importance. Although it is very difficult to conduct trials in this space, we are becoming more successful. For example, the randomized phase III SWOG 1815 trial in patients with metastatic biliary tract cancers was very successful in North America.14,16
Final Thoughts
Christopher Lieu, MD, FASCO:
The 2025 ASCO GI meeting featured a number of interesting presentations, with the BREAKWATER and the CheckMate-8HW studies, the most practice-changing right now. I would also like to mention that we saw a number of studies seeking to assess the prognostic and predictive value of circulating tumor DNA (ctDNA). We will continue to get more and more data about ctDNA and how best to use this to benefit our patients with GI malignancies.