CE / CME
Social Workers: 1.00 ASWB ACE CE Credit
Nurse Practitioners/Nurses: 1.00 Nursing contact hour
Physicians: maximum of 1.00 AMA PRA Category 1 Credit™
Released: June 02, 2025
Expiration: June 01, 2026
HCV Goals of Treatment
Of course, the next step after screening and diagnosis of HCV is treatment. The goal is sustained virologic response (SVR) or virologic cure. This is defined as a continued lack of detectable HCV RNA for 12 weeks after completing treatment, and indicates that the virus was eliminated from the body of the person who was previously infected with HCV.8,23,24
The good news is that all currently available oral regimens for HCV treatment have cure rates of up to 99% after just 8-12 weeks of treatment. Of importance, the data show similar rates of cure among individuals from all groups, including people living with HIV and people who use drugs.8,23,24
The rationale for HCV cure is manifold, with effects on the individual (both physically and emotionally), and at the population level.
At the level of the individual, there are data definitively showing that achieving cure, otherwise referred to as SVR, is associated with a reduction in liver-related mortality, reduction in the risk of subsequent hepatocellular carcinoma, and in all-cause mortality.8,23,24
On an emotional level, it can be very impactful for patients to hear that a disease they consider very stigmatizing can be cured.
In addition, HCV treatment has benefits at the population level. That is, for each person treated, the community benefits. This is reminiscent of HIV, where we have long accepted the concept of treatment as prevention. Similarly, if we reduce the reservoir of HCV in the community by decreasing the number of people with hepatitis C viremia who can potentially transmit the infection to others, we can also lower the risk of HCV acquisition for others in the community.25
MINMON: Minimal Monitoring Approach for HCV Treatment
Not only are HCV DAAs highly effective as both cure and prevention, they are simple and feasible to administer with very little clinical monitoring.
This was demonstrated by the MINMON study, which assessed the feasibility of a minimal monitoring approach for HCV treatment. In this multicenter, open-label, single-arm phase III trial, 399 participants were enrolled from more than 38 sites across more than 5 countries.
Patients enrolled in the study included individuals living with or without HIV, and individuals who did or did not report drug use.26
Patients received the entire HCV treatment course, all 84 tablets, at one time. There were no scheduled visits or lab monitoring, and there were only 2 points of remote contact, 1 at Week 4 to check in on patients, and 1 at Week 22 to schedule the Week 24 assessment to evaluate for SVR12.26
In this approach with minimal check-ins and essentially no lab monitoring, 95% of patients achieved SVR. Investigators reported that these data showed that HCV treatment is feasible with minimal monitoring in a diverse, global population.26
However, there were slightly lower rates of cure in the youngest age group, consisting of individuals from 20 to 29 years of age. The cure rate in this age group, 84.8%, is approximately 10% lower compared with the cure rates observed in the 30-59 and 60 years or older age groups. I think this shows that although all groups had very high rates of cure, some subpopulations may need a little additional support to achieve optimal HCV cure rates.26
AASLD/IDSA HCV Guidance: Simplified Treatment for Treatment-Naive Adults Without Cirrhosis
The AASLD and IDSA guidelines define 2 simplified approaches to treating HCV: one for people without cirrhosis and another for people with cirrhosis. Adults are eligible for the simplified approach for people without cirrhosis if they have chronic hepatitis C of any genotype and have not previously been treated for HCV.8
If individuals were previously treated with interferon, they still qualify for the simplified treatment algorithm. Individuals who have been reinfected are also eligible. However, it is important that they have not received prior oral DAA therapy for their current infection.8
There are 2 recommended treatment regimens when using this simplified algorithm: glecaprevir/pibrentasvir or sofosbuvir/velpatasvir. These regimens are suitable for simplified treatment because they are both pangenotypic, meaning that they are active across all HCV genotypes.8
In addition, no RAS testing is needed before starting either regimen.
AASLD/IDSA HCV Guidance: Simplified Treatment for Treatment-Naive Adults With Compensated Cirrhosis
The simplified treatment algorithm for adults with compensated cirrhosis is similar to the one for adults without cirrhosis but with additional key points.
The eligibility criteria include adults with chronic hepatitis C of any genotype who have compensated cirrhosis and who have not had prior HCV treatment for their current infection.8
Patients who are not eligible include those who have current or past decompensated cirrhosis. Typically, the term “decompensated cirrhosis” describes patients who have symptoms of liver dysfunction. This includes any prior evidence of encephalopathy, ascites, variceal bleed, or a Child-Turcotte-Pugh score ≥7.8
Patients with end-stage renal disease with an estimated glomerular filtration rate (eGFR) <30 mL/min/1.73m2 are also not eligible for this simplified treatment algorithm.
The recommended regimens for patients with compensated cirrhosis are similar to those for patients without cirrhosis, though depending on the regimen, the HCV genotype might matter.
Glecaprevir/pibrentasvir can be used with any HCV genotype.
Sofosbuvir/velpatasvir can be used with HCV genotypes 1, 2, 4, 5, or 6 without additional resistance testing.8 But if using this regimen in patients with cirrhosis with HCV genotype 3 infection, baseline NS5A RAS testing is required to assess for the presence of Y93H RAS.
This is because the rate of cure with sofosbuvir/velpatasvir drops from as high as 97% to as low as 50% in the presence of this RAS.
In patients with cirrhosis and genotype 3 infection with the Y93HRAS, the guidelines recommend either using a different regimen, such as glecaprevir/pibrentasvir, or the addition of ribavirin to sofosbuvir/velpatasvir.8
ASCEND: High SVR12 Rates With Primary-Care Professionals and Advanced-Practice Professionals
In all, the ease and efficacy of HCV treatment should enable a broad range of HCPs to provide HCV care. Early data from the oral DAA era demonstrated how effectively primary care providers and advanced-practice providers in community-based settings can administer HCV treatments.27
In this open-label, nonrandomized phase IV trial, patients were allocated to receive treatment by varying HCPs, with 150 treated by nurse practitioners,160 treated by primary care providers, and 290 treated by specialist providers. Prior to initiating HCV treatment, all HCPs received the same 3-hour training.27
Investigators reported high rates of cure among all patients, similar to those reported in clinical trials at the time. There were no statistically significant differences in rates of cure by HCP type.
Altogether, these data provide strong evidence for the effectiveness of HCV treatment provided by a broad range of HCPs in different settings.27
Task Shifting to Address Barrier of Lack of Access to Specialists
This task shifting of HCV therapy to nonspecialist HCPs can help to address the gap between the large number of patients in the United States with HCV and the low number of specialists. I think expanding provision of HCV therapy is even more important since many patients who have HCV may have challenges accessing care in specialist centers. For many such people, task shifting could be a key way to address lack of access to specialists.27-30
Many different types of HCP can deliver HCV treatment: primary care providers, addiction medicine specialists, mental health providers, physician associates, and nurse practitioners.27-30
As we expand the number of HCPs able to deliver HCV treatment, we should also think about strategies to integrate HCV treatment in a range of community-based settings. Patients can achieve high cure rates in a range of settings, including mobile to primary care, to Syringe Services Programs, to drop-in centers. We now need to embed these models of care across settings where people with HCV feel comfortable and are potentially already accessing services.27-30
When to Consult a Specialist
The reality is that the vast majority of patients infected with HCV can be treated by nonspecialists in community settings.
The scenarios in which to consider consulting a specialist are more rare, and they are listed here.8
For most patients who have no complicating conditions and whose prior DAA therapy failed, there are data suggesting that sofosbuvir/velpatasvir/voxilaprevir is effective for the treatment. However, in patients for whom multiple previous courses of prior DAA therapy have failed, referral to a specialist may be indicated.8
AASLD/IDSA HCV Guidance: Treat People Who Inject Drugs
Let us turn our attention to people who inject drugs.
CDC data suggest that up to two thirds of new HCV infections in the United States occur among people who inject drugs. This is related to the high efficiency of HCV transmission through injection drug use.31,32
To eliminate HCV as a global health threat, it is critical that we treat people who inject drugs to both improve their individual health and reduce the risk of HCV transmission to others.8
Current guidelines are clear that recent and active injection drug use are not contraindications to HCV therapy. There are no data to support additional barriers for HCV treatment initiation among people who use drugs. Enforcing pretreatment screening for drug use adds unnecessary cost, excludes a population that already feels very stigmatized by the healthcare system, and creates missed opportunities to minimize HCV transmission. HCPs should instead focus on scaling up HCV treatment efforts.8
HCV Simplified Guidance: Pretreatment Assessment
Let us shift gears and talk about how we treat HCV. The simplified guidance includes a straightforward pretreatment assessment, beginning with obtaining labs, including a complete blood count hepatic function panel, eGFR, quantitative HCV RNA, and testing for HIV and HBV because of shared modes of transmission. Among women of child-bearing age, a pregnancy test is also part of this assessment.8
Next, using data collected from the complete blood count and hepatic function panel, the guidelines recommend calculating a FIB-4 score. The FIB-4 is a tool for assessing severity of liver disease. It is critical that we know whether a patient has cirrhosis prior to treatment initiation. This determines whether there is a need for additional evaluation, such as screening for hepatocellular cancer. Cirrhosis may also affect treatment choice if the patient has a genotype 3 infection.
It is also important to perform medication reconciliation and assess for drug–drug interactions to reduce the potential of prescribing medications that are contraindicated for use together.8
Finally, patients should be educated on how to properly use their medication. I think the most important point is to reassure patients that these medications are associated with high rates of cure and that most patients will not have severe adverse effects. It is also critical to stress that if patients take the medications as recommended, with high adherence, they will likely achieve cure.8
There is, however, a risk of reinfection, and so talking about steps to take and tools to use to reduce the risk of reinfection is critical.8
HCV Simplified Guidance: On Treatment Monitoring
The vast majority of patients with HCV can be successfully treated with no laboratory monitoring required.
However, exceptions include patients taking medication for diabetes, who should be monitored for hypoglycemia, and patients taking warfarin, who should be monitored for subtherapeutic anticoagulation.8
For patients who have additional needs, including those who may have life circumstances leading to challenges with medication adherence, options to provide additional support include in-person, telehealth, or phone visits. These supportive visits can be provided by a range of personnel, including patient navigators, nurses, pharmacy staff, or peer navigators.8
Improving Access to HCV Care and Treatment
To achieve HCV elimination, we are going to have to improve access to care and treatment.
Strategies to increase access to care include incorporating peer or patient navigation services, providing culturally appropriate HCV health-related tools, materials, and information to affected communities, and providing patient education on treatment safety and effectiveness. I find that there are still individuals who think the only treatment for HCV is peginterferon-α, which was associated with significant adverse effects, and who are not aware that the new oral DAAs are highly safe and effective.7, 8,33
We also need to leverage existing resources in clinical settings to support referrals, education, and linkage to care and treatment.7,8,33
HCPs should also use approaches that partner with community-based groups that have an in-depth knowledge of the barriers and facilitators to HCV treatment uptake for the populations they serve.7,8,33
In addition, expansion of HCV treatment for incarcerated populations, who experience high rates of HCV, has potential to both significantly increase access to care and reduce rates of transmission.7,8,33
Aside from improving access to testing, improving HCV treatment itself will require providing patient and provider support in community-based settings, such as primary care clinics, opioid treatment programs, and public health clinics. Supporting HCV treatment in settings where patients are already accessing care may improve treatment outcomes.7,8,33
Similarly, better use of telemedicine can transcend geographical and temporal boundaries.7,8,33
Many people in vulnerable populations are also experiencing homelessness, transportation challenges, and food insecurity. Provision of services to help navigate these social vulnerabilities and ensure that their basic needs are met can help empower people to engage in HCV treatment.7,8,33
However, a significant barrier to HCV treatments is the cost of these medications, and the restrictions placed on treatment by insurance companies. Although challenging, removal of these restrictions will increase treatment uptake.7,8,33
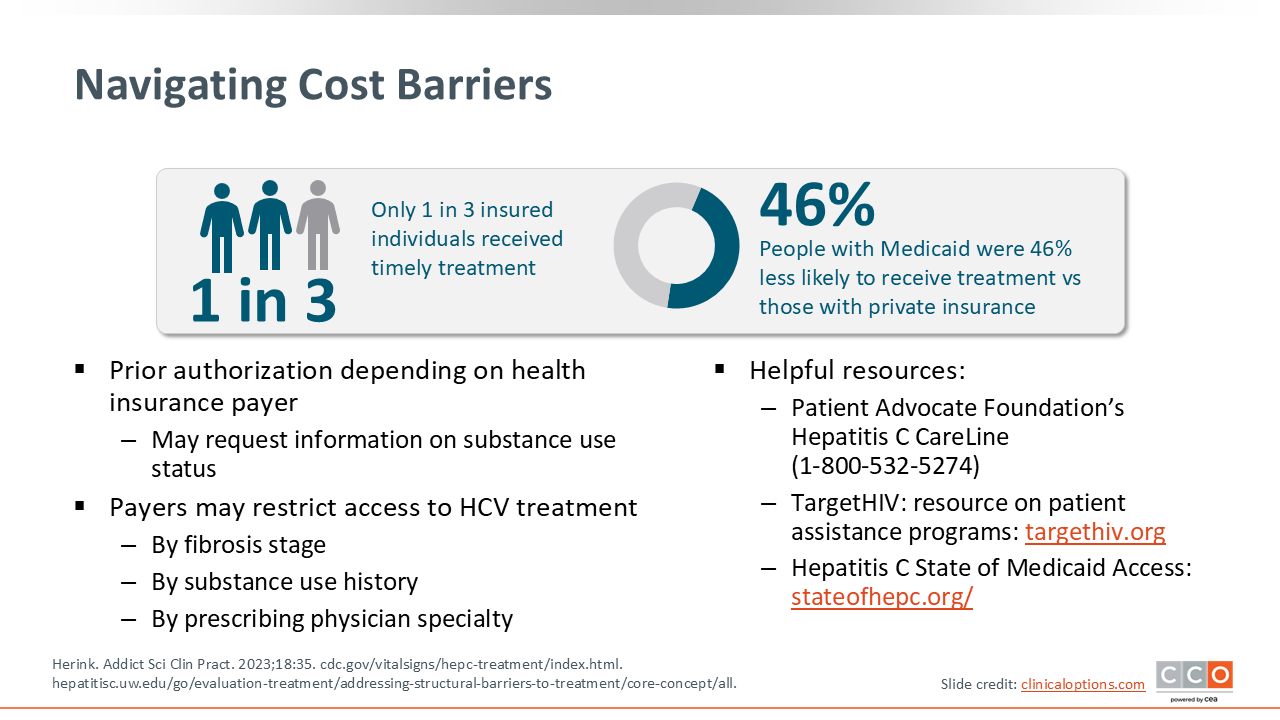
Navigating Cost Barriers
Let us delve deeper into the cost of treatment as a barrier to treatment uptake. Recent data suggest that only approximately one third of insured individuals receive HCV treatments within 6 months of diagnosis, and patients insured with Medicaid were 46% less likely to receive HCV treatment, compared with those with private insurance.34-36
Some factors that may contribute to lower treatment uptake among patients insured by Medicaid include the requirement for prior authorization, which persists in many states. Payers may also limit access to HCV treatment based on substance use, fibrosis stage, or by prescribing physician specialty.34-36
Fortunately, there are many resources to help ensure that our patients can receive HCV treatment regardless of cost, as you can see on the accompanying slide.