CE / CME
Nurse Practitioners/Nurses: 1.00 Nursing contact hour
Physicians: maximum of 1.00 AMA PRA Category 1 Credit™
Pharmacists: 1.00 contact hour (0.1 CEUs)
Released: November 22, 2023
Expiration: November 21, 2024
Approved Therapies in MDS
There is an evolving timeline of approved therapies for higher- and lower-risk MDS both in Europe by the European Medicines Agency (EMA) and in the United States by the FDA.13 The HMAs azacitidine and decitabine were the earliest approved agents for MDS, up through the recent approval of ivosidenib in 2023. In the United States, not many drugs have been approved for MDS compared with the number of approvals for other cancers, but HCPs and regulators are hopeful that this will change soon.
Mutations with targeted drug therapy in AML include IDH1/2. These mutations are less common in MDS, but their incidence increases as MDS transform.14 The FDA recently approved ivosidenib, an isocitrate dehydrogenase-1 (IDH1) inhibitor, in patients with a susceptible IDH1 mutation for the treatment of adults with relapsed or refractory MDS. Use of ivosidenib has been associated with differentiation syndrome, which can be fatal. Symptoms may include fever, hypoxia, pulmonary infiltrates, pleural or pericardial effusions, and hypotension. Management involves corticosteroid therapy, hemodynamic monitoring, and supportive care.15

Therapeutic Approach for Low-Risk MDS
Focusing on the management of patients with lower-risk MDS, clinical trial enrollment is always the preferred treatment strategy. As HCPs, we often start by looking at the cytopenia and symptom profile of the patient.
For patients with asymptomatic cytopenia, the standard continues to be observing their blood counts every few months until they become symptomatic or the cytopenia worsens significantly.
In patients who are symptomatic who have anemia, which is the most common cytopenia that happens in MDS, the standard-of-care treatment for a long time was erythropoiesis-stimulating agents (ESA,) especially if they are transfusion dependent. However, this is already changing based on results from the COMMANDS trial, which led to the 2023 approval of luspatercept for anemia in ESA-naïve adult patients with very low‒ to intermediate-risk MDS who may require regular RBC transfusions.16,17
In patients with ESA therapy failure who have ring sideroblasts or an SF3B1 mutation and have not received luspatercept previously, luspatercept is the standard of care. In patients who have del(5q), lenalidomide either before or after an ESA is also a standard option. Immunosuppression with antithymocyte globulin (ATG) with or without cyclosporine also is used, especially in patients with hypoplastic MDS.
HMA agents may be used in patients with multiple cytopenias and in patients with low-risk MDS who have isolated thrombocytopenia or neutropenia. This is not common but is always a possibility, especially if neutropenia or thrombocytopenia is severe with infections or bleeding.
Another option that is not yet approved by the FDA is thrombopoietin mimetics for patients who predominantly have thrombocytopenia as the main feature of their MDS, but only if they have lower-risk disease.18

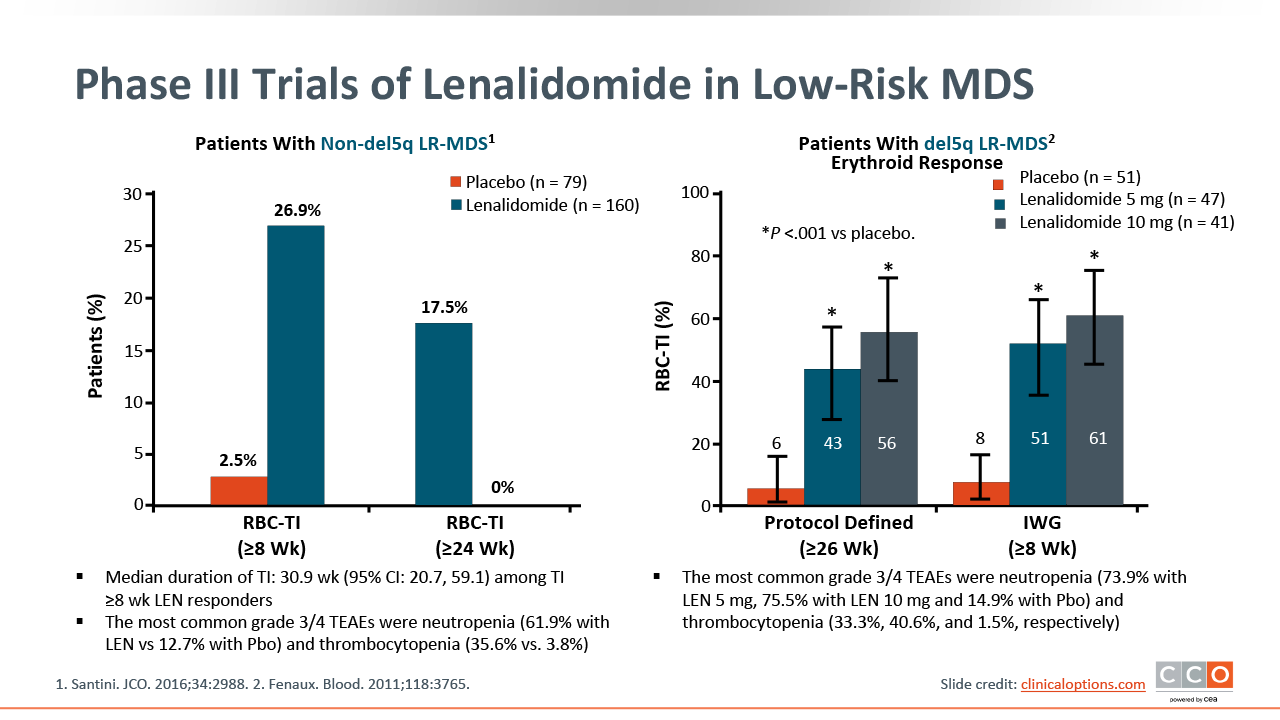
Phase III Trials of Lenalidomide in Low-Risk MDS
Several phase III trials evaluated the use of lenalidomide in low-risk MDS. Lenalidomide 10 mg and 5 mg were compared with placebo in transfusion-dependent patients with IPSS low- or intermediate-risk MDS harboring del(5q). Approximately 60% of patients achieved transfusion independence, and many of them achieved cytogenetic response.19 In another trial, lenalidomide was compared with placebo in 239 transfusion-dependent patients with IPSS low- or intermediate-risk MDS without del(5q) who were ineligible for or refractory to ESAs. Results demonstrated that patients with lower-risk MDS who do not have del(5q) still can achieve transfusion independence, but the rate is lower (27%).20 However, it is still important to consider lenalidomide as an option for patients.
Lenalidomide is an oral drug that can lead to cytopenias such as thrombocytopenia or neutropenia and other adverse events (AEs) such as fatigue and skin toxicity.21 Some patients have difficulty tolerating it, but others do well. It is important to discuss lenalidomide as an option in patients with low-risk MDS harboring del(5q).
Retrospective Study of Immunosuppressive Therapy in Low-Risk MDS
Immunosuppressive therapy, especially for younger patients or those who have hypoplastic MDS, is always a treatment option for consideration. Most studies of immunotherapy had small sample sizes. A retrospective study used information from multiple centers that offered immunosuppressants to their patients (N = 207). The predominant form of immunosuppressive treatment used in this study was ATG, which is usually synthesized from a rabbit or horse. ATG with prednisone was the most used regimen (43%). Of importance, cyclosporine monotherapy can be used in older patients who cannot tolerate ATG and in this study was used in 13% of patients. Approximately 49% of patients achieved a response, and 30% of patients achieved transfusion independence with immunosuppressive therapy.22

Low-Dose Azacitidine vs Decitabine in Low-Risk MDS
Low-dose azacitidine and decitabine are also viable treatment options. The main use of the HMAs azacitidine and decitabine is in high-risk MDS, but in lower-risk MDS—especially after failure of other modalities—lower doses of azacitidine and decitabine have led to transfusion independence in some patients. A phase II trial randomly assigned 113 treatment-naive patients with MDS with an IPPS risk of low or intermediate-1 to receive low-dose azacitidine or decitabine. The ORRs were 48% and 67% with azacitidine or decitabine, respectively. Approximately 32% of patients with baseline transfusion dependence reached transfusion independence. With short courses of these drugs, responses can be durable. The median duration of transfusion independence in this specific study was approximately 22 months.23 Treatment with low-dose HMA was well tolerated in both arms, with rare grade ≥3 AEs. Infection or neutropenic fever occurred with azacytidine (7%) and decitabine (5%) treatment.24

MEDALIST Phase III Trial of Luspatercept
In low-risk MDS, anemia is a major clinical problem and can be associated with complications such as fatigue and cardiac problems, especially in older patients. Many patients with low-risk MDS become transfusion dependent.25 The ESAs erythropoietin and darbepoetin alfa have been shown in trials to reduce or eliminate transfusion need in approximately 60% of patients, especially in those who have a low transfusion burden and/or a low erythropoietin level.26 However, all patients, even if they respond to ESAs initially, eventually will stop responding after 12-18 months.
Luspatercept is a ligand trap; it removes ligands of the transforming growth factor β pathway. These ligands circulate and activate SMAD2/3 signaling, which suppresses late-stage erythropoiesis. Luspatercept interferes with this activation and leads to restoration of erythropoiesis. The phase III MEDALIST trial compared luspatercept with placebo in 229 transfusion-dependent patients with low- or intermediate-risk MDS refractory to or unlikely to respond to ESAs. The primary endpoint of ≥8 weeks of transfusion independence during the first 24 weeks was observed in 38% and 13% of patients who received luspatercept and placebo, respectively (P <.001).25
Based on these results, luspatercept was approved for anemia failing an ESA and requiring ≥2 RBC units in 8 weeks in adult patients with very low‒ to intermediate-risk MDS with ring sideroblasts or with myelodysplastic/myeloproliferative neoplasm with ring sideroblasts and thrombocytosis.16

MEDALIST: Luspatercept vs Placebo Hematologic Outcomes
In a longer-term follow-up analysis of the MEDALIST trial, it was demonstrated that patients not only benefit from transfusion independence, but there also is significant reduction in the RBC transfusion burden. In 48 weeks, 58.8% of patients receiving luspatercept achieved a modified hematologic improvement‒erythroid response vs 17% in the placebo arm (P <.001.) There was erythroid hematologic improvement regardless of transfusion burden severity.27

COMMANDS: Luspatercept vs Epoetin Alfa in Lower-Risk MDS
In the phase III COMMANDS trial, luspatercept was tested as a frontline agent vs epoetin alfa in patients who were transfusion dependent with lower-risk MDS and endogenous erythropoietin <500 U/L. Patients (N = 356) were randomized to receive luspatercept or epoetin alfa until progressive disease. The primary endpoint was RBC transfusion independence ≥12 weeks with a concurrent mean hemoglobin increase of ≥1.5 g/dL.17

COMMANDS Transfusion Independence
After a median treatment duration of 42 weeks, 59% of patients receiving luspatercept achieved RBC transfusion independence combined with a hemoglobin increase of ≥1.5 g/dL vs 31% of patients on the ESA arm (P <.001). The beneficial effect of luspatercept was observed across different subgroups, including baseline erythropoietin level, baseline transfusion burden, and SF3B1 mutation status. In patients who did not have ring sideroblasts, the transfusion independence rate appeared similar, but the durability was longer with luspatercept vs ESA.17

COMMANDS AEs
In terms of AEs, there were no new concerning features compared with the previously reported MEDALIST data. The AEs were well balanced between luspatercept and epoetin alfa. Of importance, there was no difference in progression to MDS or AML, and most AEs were grade 1-2 in severity. Grade 3 AEs were relatively rare, with fatigue and gastrointestinal issues among the most common.17,28

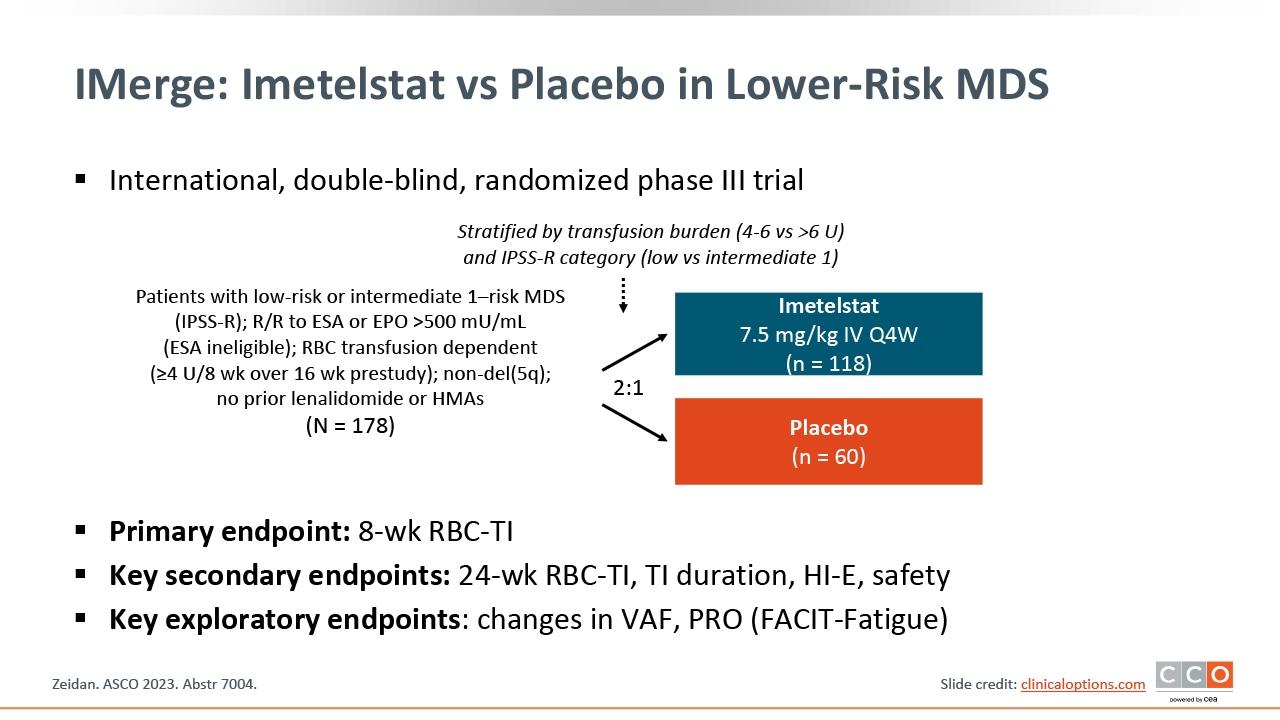
IMerge: Imetelstat in Lower-Risk MDS
Imetelstat is another promising investigational agent for lower-risk MDS. It is a first-in-class telomerase inhibitor that binds to the RNA template of telomerase and inhibits enzymatic activity. It has been shown to target malignant clones with high telomerase activity, which leads to the induction of apoptosis.29
The phase II portion of the IMerge study evaluated imetelstat in 57 transfusion-dependent patients with low-risk MDS who were ineligible for or relapsed/refractory to ESA treatment. The 8-week transfusion independence rate was 37%. A subset population of 38 patients who were lenalidomide naive showed 42% with 8-week transfusion independence.30 Based on these findings, the phase III IMerge study was conducted.
The phase III IMerge study portion was an international, double-blind, randomized trial that assigned transfusion-dependent patients with low-risk MDS who were ineligible for or relapsed/refractory to ESAs to receive imetelstat or placebo. The transfusion dependency requirement before enrollment was that patients were required to receive ≥4 units of blood in 8 weeks, so they were heavily transfused at baseline.31
IMerge: Transfusion Independence Over Time
The transfusion independence rate was 39.8% vs 15.0% at 8 weeks with imetelstat vs placebo (P <.001). Responses were durable, with a median duration of response of nearly 52 weeks. A single continuous transfusion independence period was achieved in 83% of 8-week responders to imetelstat.31

IMerge: Duration of Transfusion Independence
The duration of transfusion independence was 51.6 weeks with imetelstat vs 13.3 weeks with placebo (P <.001).31

IMerge: Hemoglobin Responses
There was an increase in the mean hemoglobin increase of 3.6 g with imetelstat vs 0.8 g with placebo. The patients who were responding to imetelstat treatment had improved and increased hemoglobin levels over time.31

IMerge: Cytopenias
The most common AEs observed with imetelstat were neutropenia and thrombocytopenia, which were mostly grade ≥3 and occurred within the first few cycles. However, most of those cytopenias were reversible with treatment delays, treatment reduction, and growth factor use. In fact, ≥80% of the neutropenia and thrombocytopenia resolved to grade ≤2 within 2 weeks with treatment adjustment. Clinical ramifications related to severe thrombocytopenia or neutropenia did not increase, meaning that clinically significant bleeding or severe infections resulting from thrombocytopenia or febrile neutropenia did not differ between the 2 arms. This finding suggests that thrombocytopenia and neutropenia can be mitigated well with proper monitoring and management.31

IMerge: Most Common AE
Nonhematologic AEs were mostly low grade. They included asthenia, COVID-19, and headache. Most patients (~75%) receiving imetelstat had dose modifications because of AEs, and <15% discontinued treatment because of AEs. There were no cases of treatment-related liver injury or Hy’s law liver toxicity. Aside from this, most of the AEs observed on the trial were grade 1/2 and were manageable.31